
All the possible effects of the NRP on public health

The article by Pietro Gonella and Stefano Biasioli
The Covid pandemic seems to have stirred the waters, in Europe and in Italy. It took at least 150,000 Italian deaths, directly or indirectly induced by Covid, to induce Europe first and the Italian government (later) to provide specific funding within the PNRR for a drastic reform of the Italian NHS , dated 1978 and with few tweaks since then.
In a recent article we recalled that, for at least 25 years, we have been fighting for a modernization of the NHS, aimed at avoiding its downgrading, due to the evident inability of the health facilities provided and created by law 833 (1978-2021) to facing the new health needs and the dramatic change in the most serious and resource-consuming diseases.
The tragedy of Covid – and the clear European guidelines – have led Draghi to elaborate, within the PNRR, a draft of health care reform, with specific funding of about 19-20 billion, although much more would be needed (at least 32) .
The innovations of the NRP can be summarized in some 4 fundamental elements:
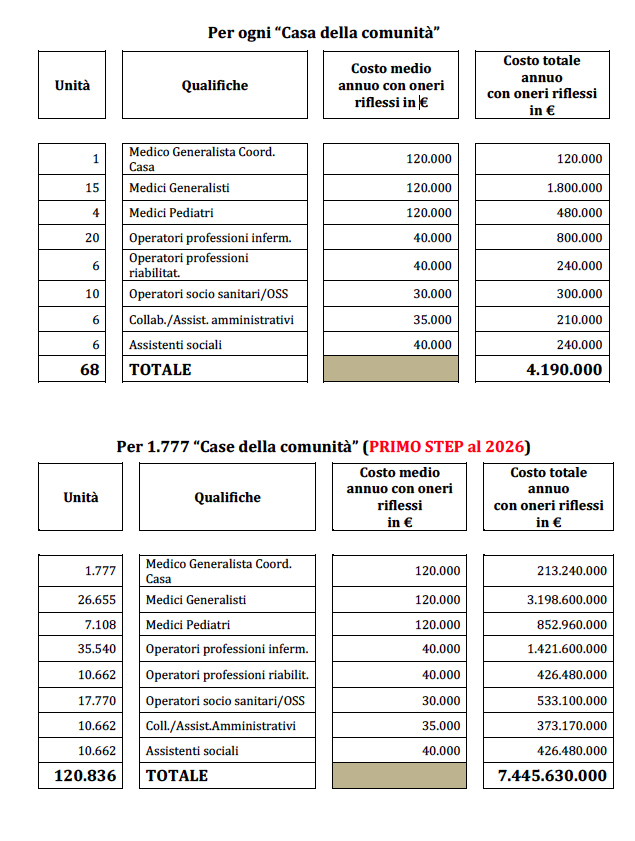
to. "Community Houses" (1 per 20,000 inhabitants) – Standard 3,010.
Now 459 are active. As the first step, another 1,288 must be activated by 2026 for a total of 1,777 “Houses”. And the remaining 1,233 “Houses” to reach the Standard? What second step will they be activated by 2.030?
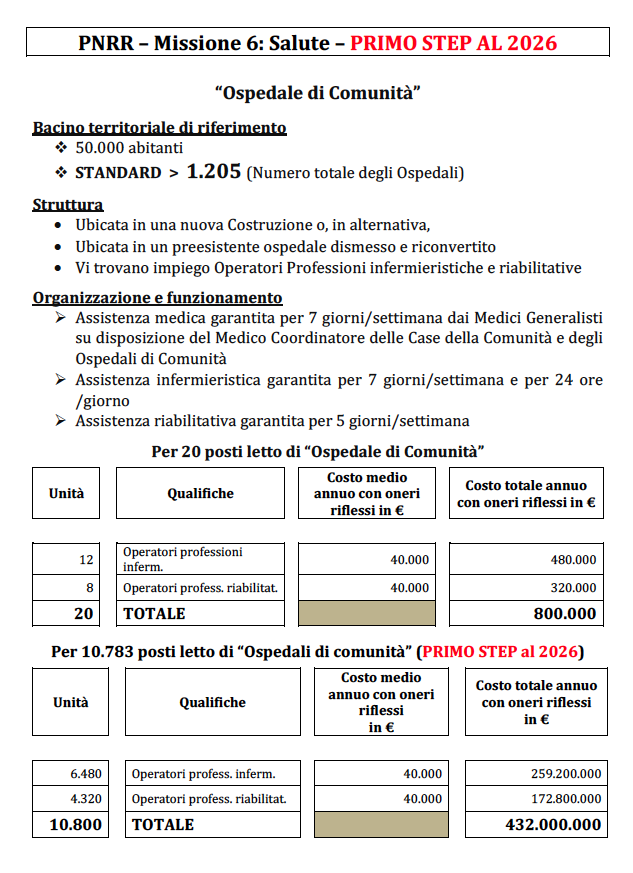
b. "Community hospitals" (1 for every 50,000 inhabitants) – Standard 1,205.
3,163 beds are now active. 381 "Hospitals" must be activated, for a total of additional 7,620 beds (381 x 20 beds), for a total of 10,783 beds as a first step
And the remaining 13,317 beds to reach the Standard? Is it a total of 24,100 beds (1,205 x 20 beds), a number that requires the activation of another 665 “Hospitals”? What second step will they be activated by 2.030?
c. "Home care" (for 1,500,000 inhabitants, or 10% of over 65s). About 702,000 patients are now followed at home (5.1% of those over 65).
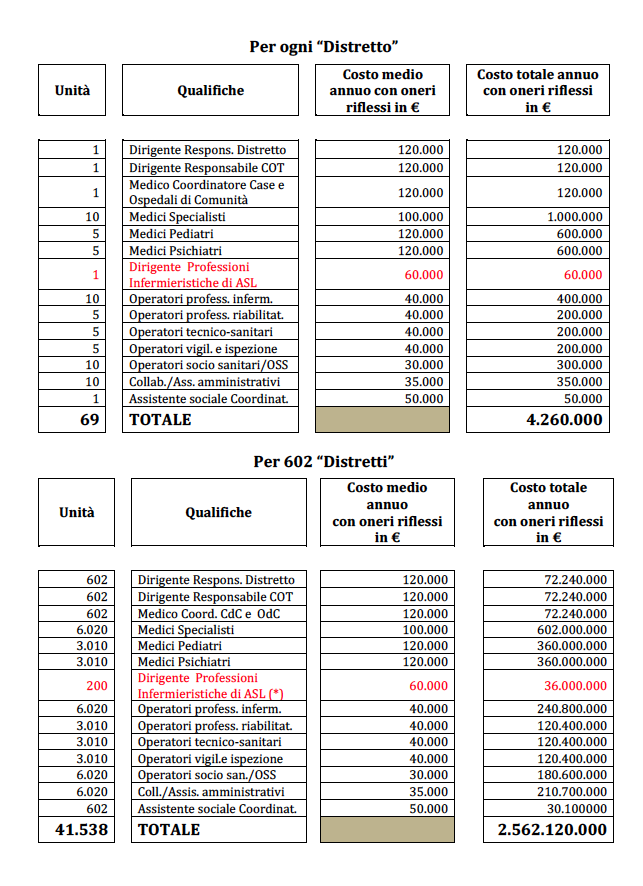
d. “Territorial Operations Centers” (1 per 100,000 inhabitants), therefore 602 corresponding to the Territory of each District.
A huge task, to be carried out – as a first step – from 2022 to 2026, in just 5 years. This is why the writer has decided to put pen to paper and to quantify not so much the incompressible structural expenses, but to define – once and for all – the annual costs of the personnel, medical-health and technical personnel essential to make the aforementioned 4 work. assistance modalities, realized that the necessary structures are.
The quantification of these costs – in relation to the first step – was made by one of us, as head of the management of the NHS personnel at the time, with ten-year experience in Coordinating the General Managers of ASL / AULSS. The tables are available at the end of the article, structured in analytical items. They are based on the fundamental concept that, in order for them to function, they must have all the personnel necessary for a “correct functioning when needed”, without a priori cuts to the same / staffing.
In summary, here are the annual personnel costs (including reflected charges):
- COMMUNITY HOUSES: 1 for every 20,000 inhabitants, each with 68 professional figures and with annual costs of 4,190,000 euros / year. The total expenditure for 1,777 such houses would therefore be 7.445630 billion euros / year. About 4.5 billion euros / year are currently already supported by the budgets of the ASLs. Therefore, approximately 3 billion euro / year remain to be covered. But the government project on the Recovery fund finances this point with 2 billion, in 5 years….!
- COMMUNITY HOSPITALS: 1 for every 50,000 inhabitants, each with 20 beds and 20 operators; annual staff cost = 800,000 euros / hospital. With the creation by 2026 of another 7,620 new beds for a total of 10,738 beds (in new buildings or in pre-existing abandoned hospitals), a staff cost of around 432 million euros / year will have to be incurred. But the Recovery fund provides a loan of 1 billion over 5 years…!
- DISTRICT / HOME CARE: 1 per 100,000 inhabitants, each with 69 units and with a staff cost of 4,260,000 euros / year. For 602 “Districts”, the total is 2.562120 billion euros / year. On this point too, the Recovery fund provides for a loan of 4 billion over 5 years….!
It is necessary to know that, within the district (or on the side?), The TERRITORIAL OPERATIONAL CENTER (COT), in charge of coordinating the various territorial services, must be totally modified. The cost of the related personnel has already been entered by us in item 3, but the costs relating to: new hardware, new software, new connection systems with the 3 previously mentioned structures should be calculated and quantified separately, to really create a full connection "Health" within a province and on at least a regional basis. This requires technological innovation, a transformation of the health card from "passive" (mute microchip) to "active" (microchip loaded with basic clinical information of the patient), personnel adequately informed and active 24 hours a day, 7 days a week.
Taking 4 accounts, the personnel expenditure would be equal to at least 10 billion euros / year. Taking into account that 6 billion are currently already supported by the budgets of the ASLs, there are 4 billion euros / year left which obviously would be added to the annual expenditure currently incurred by the NHS. Because, in this case, reorganization would not mean containment of territorial expenditure but an expansion of the same also through a partial transfer of resources from the hospital sector. Obviously this, for us, should take place not to the detriment of emergency hospitals, clearly in crisis in 2020-2021, because they are underestimated compared to the European average and compared to a serious emergency, what the Covid pandemic was and still is.
We wonder if Prime Minister Draghi and "his" control room are aware of this and what is the articulated plan for 2022-2026 to concretely respond to European prescriptions. Which weigh more than the "leaflets" included in the packaging of drugs …
Finally, there remains the enormous chapter of the contractual aspects of all healthcare personnel.
On the point relating to family doctors (GPs) we think exactly like Professor Remuzzi: they must be transformed into dependent doctors, abandoning the atypical current figure of "affiliated doctors", self-managed. Yes, a nice boulder, this …
This is a machine translation from Italian language of a post published on Start Magazine at the URL https://www.startmag.it/sanita/tutti-i-possibili-effetti-del-pnrr-in-tema-di-sanita-pubblica/ on Sat, 12 Jun 2021 05:28:31 +0000.